




Introduction
If you have ever been diagnosed with polycystic ovary syndrome, the first question most people ask is: do I actually have cysts on my ovaries? It is a reasonable question given the name. The answer, for most people, is no. And that confusion, repeated across millions of consultations over decades, is exactly why a landmark global consensus published in The Lancet in May 2026 has formally renamed the condition. Polycystic ovary syndrome is now called polyendocrine metabolic ovarian syndrome, shortened to PMOS.
This is not a rebranding exercise. It is a correction that has been needed for a very long time.
What Was Wrong with the Old Name
The term polycystic ovary syndrome implies the presence of pathological ovarian cysts. These cysts are not actually a feature of the condition. What is seen on ultrasound in many affected individuals is an accumulation of small, immature follicles that have failed to develop properly. That is a completely different thing from pathological cysts, and the name has been creating confusion about this distinction since the condition was first described.
Beyond that specific inaccuracy, the name frames a complex, multisystem condition as though it is primarily an ovarian problem. It is not. The ovaries are affected, but they are not where the condition originates or where its most significant health consequences play out. Describing the full picture of this condition using only the word polycystic and the word ovary leaves out the hormonal disturbances, the metabolic complications, the cardiovascular risk, the psychological impact, and the dermatological features that are all part of how this condition actually presents.
The consequences of this naming failure have been significant and measurable. Up to seventy percent of people with this condition remain undiagnosed. Patients consistently report confusion about what the condition is and dissatisfaction with how it is explained and managed. Clinicians working outside reproductive medicine have historically underrecognised it because the name pointed toward a single specialty rather than signalling the multidisciplinary attention the condition requires. Research classification and health system coding have been complicated by the same inaccuracies. A misleading name has real downstream costs for real people.
What the Condition Actually Involves
To understand why the new name is more accurate, it helps to understand what this condition actually is.
PMOS is first and foremost a hormonal condition involving multiple endocrine systems at once. The prefix polyendocrine in the new name reflects this. It is not one hormone that is disrupted. It is several, interacting with each other in ways that produce a wide range of symptoms and health consequences.
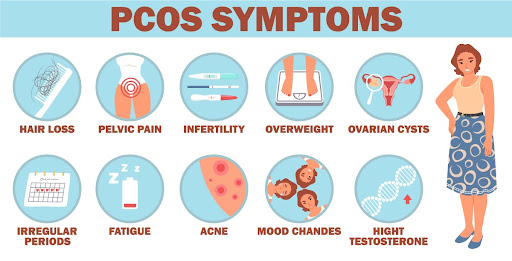
Elevated androgens, which are hormones typically thought of as male hormones but present in all bodies, are a defining feature. These come from both the ovaries and often the adrenal glands. Elevated androgens are responsible for symptoms like excess facial or body hair, acne, and hair thinning on the scalp. They are also connected to the metabolic features of the condition.
Insulin resistance is present in the vast majority of people with PMOS. Importantly, this includes around seventy-five percent of people with PMOS who have a lean body weight, meaning this is not simply a consequence of weight. When the body becomes resistant to insulin, it compensates by producing more of it. Higher insulin levels in turn stimulate further androgen production from the ovaries, creating a cycle that worsens both the hormonal and metabolic features of the condition simultaneously.
The metabolic consequences of PMOS are serious and extend well beyond blood sugar. People with PMOS have increased rates of impaired glucose tolerance, type 2 diabetes, gestational diabetes during pregnancy, liver disease, abnormal cholesterol levels, high blood pressure, and cardiovascular disease. The research shows that the odds of composite cardiovascular disease are around 1.68 times higher in people with PMOS compared to those without the condition. The risk of heart attack is 2.5 times higher and the risk of stroke is 1.71 times higher. These are not marginal statistics. They describe a condition with real and serious long-term health implications that go far beyond reproductive function.
The ovarian involvement is also real and clinically important. The hormonal disruption impairs the normal development of follicles in the ovaries, leading to irregular or absent ovulation, menstrual irregularity, and infertility. Elevated anti-Müllerian hormone, a marker of ovarian function now included in the diagnostic criteria for adults, reflects this disrupted follicular development. The term ovarian in the new name captures these features more accurately and more completely than ovulatory would, because ovarian encompasses the endocrine and structural dimensions of what is happening in the ovaries, and because ovulatory becomes an incomplete description after menopause.
Beyond the hormonal, metabolic, and ovarian features, the condition is also associated with significant psychological consequences. Depression, anxiety, eating disorders, and reduced quality of life are well documented in people with PMOS and are considered part of the clinical picture, not separate concerns.
The dermatological features, including acne, excess hair growth, and scalp hair thinning, are also part of the condition and largely follow from the androgen excess rather than representing an independent process.
How the New Name Was Chosen
The process behind choosing the new name was extensive, rigorous, and deliberately inclusive. It is worth understanding how it worked because the credibility of the name change rests on the quality of the process that produced it.
The global effort involved 56 leading academic, clinical, and patient organisations from across all world regions. Two rounds of global surveys were conducted, generating over 14,000 responses from people living with the condition and from multidisciplinary health professionals including specialists in obstetrics and gynaecology, endocrinology, reproductive medicine, primary care, nutrition, nursing, paediatrics, dermatology, and psychology. Two rounds of international consensus workshops were held, using established methods designed to generate legitimate and transparent group decisions. A marketing and communications analysis was conducted to assess candidate names for clarity, cultural appropriateness, and practical feasibility of adoption.
People with the condition were not just surveyed. They were involved in governance, in the design of the surveys, in the facilitation of workshops, and in the development of the implementation strategy. Their input was treated as essential rather than supplementary.
The guiding principles for the new name were established early and held consistently throughout. The name needed to be scientifically accurate, clearly communicable, free from stigmatising language, culturally appropriate across diverse contexts, and practically implementable within existing health systems and research frameworks.
Several candidate names were considered and ruled out for specific reasons. One was eliminated because its acronym would have duplicated the abbreviation for a completely different respiratory condition. Another was found to overlap in its acronym with a well-known youth subculture in ways that would have created confusion in clinical and public communication. The process of elimination was evidence-based and documented at every stage.
The final name, polyendocrine metabolic ovarian syndrome, emerged from this process as the one that best satisfied all the agreed principles. Eighty-six percent of patients and seventy percent of health professionals in the surveys supported adopting an accurate, symptom-based name. The specific terms polyendocrine, metabolic, and ovarian each reflect a distinct and scientifically grounded aspect of the condition. Taken together they describe what the condition actually is in a way that polycystic ovary syndrome never did.
What Actually Changes
The condition itself does not change. The biology is the same. The diagnostic criteria are the same. If you were diagnosed with PCOS, you have the same condition now called PMOS. No rediagnosis is required and no existing management plan becomes invalid.
What changes is how the condition is named, described, framed, and ultimately understood. A name shapes what clinicians look for, what they explain, what they prioritise in treatment, and how patients understand their own health. An accurate name is itself a clinical intervention.
The implementation process is designed as a managed evolution over three years rather than an abrupt replacement. The strategy includes academic dissemination, the development of multilingual resources for patients and clinicians, integration into electronic health records, engagement with governments and research funding bodies, formal engagement with the World Health Organization for integration into international disease classification codes, and planned incorporation into the International Guidelines update scheduled for 2028, which are currently used in 195 countries.
Why This Matters
One in eight women globally is affected by this condition. It is one of the most common endocrine conditions in women of reproductive age. It has cardiovascular, metabolic, reproductive, psychological, and dermatological consequences that span a lifetime, including beyond the reproductive years during which the condition is most commonly diagnosed.
For decades, the name has obscured what the condition is, delayed how quickly it is recognised and diagnosed, narrowed how it is treated, and contributed to stigma in contexts where the reproductive language carries particular cultural weight. Getting the name right is not a cosmetic change. It is the foundation for getting everything else right: the diagnosis, the care, the research, the policy, and the lived experience of the millions of people managing this condition every day.
The condition now has a name that reflects what the science actually says. That is what the science was always pointing toward.
Reference:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext